
Patients expect care that is responsive, coordinated, and clear whether they’re booking an appointment, checking benefits, requesting a refill, or managing a chronic condition. Teams, meanwhile, navigate high volume, workforce shortages, complex rules, and tight reimbursement. The fastest‑growing solution set sits at the intersection of workflow and intelligence: AI agents in healthcare automation.
Done right, these systems reduce delays, prevent errors, and free clinicians and staff to do the work only humans can do. Done poorly, they create risk. This guide shows how to plan, build, buy, and govern AI agents in healthcare automation responsibly so you earn trust, safeguard privacy, and deliver measurable results.
What you’ll learn:
- What AI agents in healthcare automation are and where they add real value
- End‑to‑end use cases across access, care delivery, revenue cycle, and pharmacy
- Integration patterns for EHRs, payers, and partner systems (FHIR, HL7, X12)
- Safety, privacy, and regulatory guardrails (HIPAA, 42 CFR Part 2, FDA/SaMD, EU AI Act)
- A 90‑day rollout plan, ROI modeling, KPIs, and operating rhythms that stick
- Common pitfalls to avoid, plus case snapshots and future trends
This article is for informational purposes and does not constitute medical, legal, or regulatory advice. Always involve your compliance and clinical leadership when deploying automation that touches patient journeys.
What are AI agents in healthcare automation?
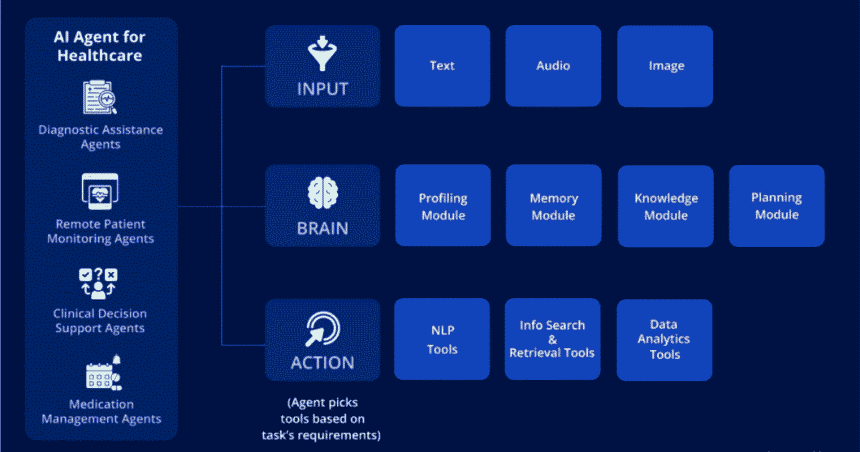
At their core, AI agents in healthcare automation are goal‑oriented software assistants that can understand requests, retrieve context from clinical and operational systems, follow policy‑bound steps, take safe actions, and escalate to people when needed. Think of them as workflow teammates:
- Understand: Interpret natural language in patient or staff messages; detect intent and sentiment
- Retrieve: Pull facts from the EHR, payer portals, policy libraries, and past interactions
- Decide: Choose the next best action under clear rules (benefits check, prior authorization steps, scheduling slots)
- Act: Execute via approved tools verify eligibility, assemble clinical documentation, submit claims, reschedule visits
- Learn & escalate: Incorporate feedback; hand off to a human with a clean summary when confidence is low or rules require oversight
These agents don’t replace clinicians or staff. They handle repetitive, rules‑driven work and prepare perfect handoffs on everything else. The more policy‑rich and data‑bound a task is, the more an agent can help.
The business case: Why adopt AI agents in healthcare automation now
Leaders lean in for three reasons: access, quality, and economics.
- Access and experience
- 24/7, multilingual self‑service for routine needs
- Lower wait times and faster callbacks
- Clearer communication reduces confusion and no‑shows
- Quality and safety
- Consistent steps and documentation (fewer misses)
- Earlier detection of risks (e.g., gaps in care, therapy conflicts)
- Reliable follow‑through on referrals, labs, and monitoring alerts
- Economics and workforce
- Lower cost per task (eligibility checks, prior auth, claim scrubbing)
- Reduced denials and faster revenue cycles
- Less after‑hours administrative burden for clinicians; lower burnout
A simple ROI model:
- Annual task volume (V); automation (containment) rate (C%)
- Human cost per task (H); automated cost per task (A)
- Annual savings = V × C% × (H − A)
- Add revenue lift from recovered leakage (kept appointments, reduced denials)
- Net ROI = (Savings + Revenue lift − Program costs) ÷ Program costs
Even modest containment (20–40%) on high‑volume workflows often yields outsized returns when paired with fewer errors and faster cycle times.
Where AI agents in healthcare automation add the most value
Below are high‑impact use cases across the care continuum, grouped by domain. Each benefits from explicit policies, reliable integrations, and clear escalation rules.
1) Digital front door and patient access
- Symptom guidance and routing (non‑diagnostic):
- Capture reason for visit, red flags, and preferred times; route to the right level of care
- Safety: disclaimers; escalation to nurse triage if concerning symptoms emerge
- Appointment scheduling and rescheduling:
- Read/write access to visit types, providers, and slots; confirm insurance network status
- Reduce abandoned calls; send prep instructions automatically
- Benefits and cost clarity:
- Verify eligibility (X12 270/271), estimate out‑of‑pocket based on plan rules and historical allowed amounts
- Present alternatives (in‑network facilities, virtual options)
- Referrals and pre‑visit readiness:
- Gather intake forms, medications, allergies, and consents before the visit
- Nudge completion via SMS/email; update EHR and patient portal
Why it works: These tasks are structured, policy‑heavy, and frequent ideal for AI agents in healthcare automation.
2) Clinical documentation and care coordination
- Ambient note support:
- Summarize patient‑clinician conversations into HPI/ROS/Exam/Plan
- Draft notes for clinician review; map terms to SNOMED CT/ICD‑10 where appropriate
- Orders and results tracking:
- Ensure labs and imaging orders are scheduled; notify patients on critical results with escalation to clinician
- Reduce “orders placed, not done” leakage; improve safety follow‑through
- Care gap closure:
- Identify open quality measures (e.g., A1c, colon screening); schedule and remind
- Coordinate with care managers; document outreach and outcomes
- Transitions of care:
- Summarize discharge instructions; coordinate follow‑ups and referrals
- Confirm home health setup, DME delivery, and medication reconciliation
Why it works: AI agents in healthcare automation excel when knowledge of policies, timelines, and roles governs the next step.
3) Pharmacy and therapy support
- Medication reconciliation:
- Pull from Rx histories (NCPDP, Surescripts), EHR med list, and patient input; flag duplicates, interactions, or adherence risks
- Refills and renewals:
- Capture requests; check last fill and lab requirements; draft renewal for clinician sign‑off
- Prior authorization (ePA):
- Assemble documentation from notes, labs, and imaging; submit to payer; track status; alert when additional info is requested
- Adherence nudges and side‑effect triage:
- Reminders timed to patient routine; capture issues; route to pharmacist or clinician when needed
Why it works: High volume, policy‑bound steps perfect for AI agents in healthcare automation with strong guardrails.
4) Revenue cycle and financial clearance
- Eligibility and coverage discovery:
- Verify active coverage; identify secondary insurance; reduce “self‑pay” errors
- Claim scrubbing and coding assist:
- Flag missing modifiers, diagnosis‑procedure mismatches, or NCCI edits before submission
- Denial management:
- Classify denial reasons; auto‑draft appeals with supporting documentation; route complex cases to specialists
- Estimates and financial counseling:
- Generate uncomplicated estimates with clear disclaimers; offer payment plans; capture consent
Why it works: Rules are explicit; outcomes are measurable AI agents in healthcare automation shine in these repetitive, high‑stakes processes.
5) Remote monitoring and chronic condition support
- RPM alert triage:
- Filter and prioritize device alerts (BP, glucose, SpO2) using patient‑specific thresholds
- Ask clarifying questions via portal/SMS; notify clinician for concerning trends
- Care plan adherence:
- Provide nudges and micro‑education; track completion; celebrate progress
- Route to care manager on persistent non‑adherence
- Social needs follow‑up:
- Screen for food, housing, or transportation barriers; refer to community resources; document outcomes
Why it works: Always‑on follow‑through is what AI agents in healthcare automation do best freeing clinicians from constant manual checks.
Architecture: how to build reliable AI agents in healthcare automation
A production‑grade design separates concerns: understanding, context, action, and safety.
Core components
- Channel adapters:
- Phone/IVR, SMS, chat, patient portal, email
- Normalize messages; attach identity and encounter context
- Orchestrator:
- Detect intent and entities (order ID, plan name, symptoms)
- Plan steps under policies; decide to act, ask, or escalate
- Retrieval and grounding:
- Knowledge bases (policies, procedures, patient education)
- Clinical/operational data (EHR via HL7 v2 and FHIR R4/R5; scheduling; billing; labs; imaging)
- Payer/clearinghouse (X12 270/271, 278, 837/835)
- Vector indexes for semantic search over internal content
- Tool connectors:
- EHR write APIs (SMART on FHIR, Bulk/B2B, vendor REST)
- Scheduling, RCM, prior auth, pharmacy, telephony, CRM
- Idempotent actions with retries and timeouts
- Safety and governance:
- PII redaction/masking by default; encryption in transit/at rest
- Allow/deny lists; parameter validation; rate limits
- Approvals for high‑risk actions (e.g., changing care plans, large refunds)
- Immutable audit logs with full traceability
- Human‑in‑the‑loop:
- Confidence thresholds; clear escalation paths
- Summaries and recommended next steps for clinicians or staff
- Feedback capture to improve policies and content
- Observability:
- Tracing, metrics (p50/p95 latency), error taxonomy, cost dashboards
- Quality review queues; golden test sets for regression checks
Design principle: Make the “happy path” fast, and the “unhappy path” safe especially when protected health information is involved.
Integration patterns that work (and what to watch)
- EHR and clinical systems:
- HL7 v2 (ADT, ORU, SIU) for legacy feeds; FHIR APIs for read/write (Patient, Appointment, ServiceRequest, CarePlan, Observation, MedicationRequest)
- SMART on FHIR (OAuth 2.0) and Backend Services for server‑to‑server access
- Identity: Master Patient Index (MPI); careful matching and deduplication
- Payer and RCM:
- X12 transactions (270/271 eligibility, 278 prior auth, 837 claim, 835 remittance)
- Attachments (HL7 / X12 275) for clinical documentation
- Clearinghouses for connectivity and status normalization
- Telephony and messaging:
- IVR/CCaaS platforms for routing and transcription; SMS gateways with opt‑in/opt‑out handling
- Consent management and quiet hours rules
- Knowledge and content:
- Policy wikis, clinical protocols, patient education libraries (mapped to LOINC/SNOMED where applicable)
- Content versioning and review workflows
Watch‑outs:
- Write access is power enforce least privilege and approvals
- Monitor for data drift; retire stale content
- Ensure idempotency (e.g., avoid duplicate orders or claims)
Safety, privacy, and regulatory guardrails
Trust is non‑negotiable. Bake these controls into your AI agents in healthcare automation from the start.
- HIPAA and 42 CFR Part 2:
- Minimum necessary access; audit logs; BAAs with vendors
- Special handling for substance use disorder records (Part 2)
- Authentication and authorization:
- SSO for staff; strong identity verification for patients before account changes
- Role‑based access; separation of environments; key rotation
- FDA and SaMD (U.S.):
- Determine if the function is medical device software (diagnostic, treatment recommendations) vs. non‑device support (administrative, documentation)
- For device‑like functions, follow applicable FDA pathways (e.g., 510(k)); apply ISO 14971 (risk), IEC 62304 (software lifecycle), IEC 62366 (usability)
- ONC and decision support transparency:
- For EHR‑connected decision support, align with ONC’s expectations for data provenance and transparency (HTI‑1 rule and DSI provisions)
- EU AI Act and MDR:
- Classify use cases appropriately; high‑risk medical functions require documentation, risk management, and oversight
- Data ethics and fairness:
- Measure performance across demographics and languages; mitigate bias
- Provide accessible alternatives and support for people with disabilities (Section 1557, ADA)
- Content and action safety:
- Deny list for unsafe actions; parameter checks (e.g., patient belongs to encounter, dosages within bounds if agents surface options for clinicians)
- Escalate when uncertainty is high; never fabricate clinical facts
If it’s not safe, it’s not shippable especially for AI agents in healthcare automation.
Implementation playbook: your first 90 days
A disciplined rollout reduces risk and shows value fast.
Days 1–30: Foundation
- Pick two to three high‑volume, low‑risk workflows
- Examples: eligibility verification, appointment rescheduling, order/result follow‑up
- Define success:
- What counts as “resolved”? Target containment, p95 latency, escalation rules, and CSAT
- Clean your knowledge base:
- Remove stale content; add decision trees and step‑by‑step guides
- Map tools and approvals:
- Which actions are permitted? Who approves exceptions?
- Stand up guardrails:
- Redaction, policy engine, rate limits, kill switches, audit logs
- Build a golden test set:
- 200–500 real examples with correct outcomes to validate changes
- Create dashboards:
- Containment, TTR, CSAT, escalation reasons, safety events
Exit criteria: end‑to‑end tests pass in sandbox; go‑live plan agreed.
Days 31–60: Pilot
- Start with chat or portal messages (lower risk than voice)
- Shadow mode:
- Agents draft responses; humans send. Compare results and fix gaps
- Canary rollout:
- 10–20% live traffic on chosen workflows; expand as metrics hold
- Weekly quality rounds:
- Review transcripts; update policies and content; fix tooling gaps
- Train staff:
- Supervision, escalation, and how to provide actionable feedback
Exit criteria: containment ≥30% on scoped workflows; CSAT within 5% of baseline; zero critical policy violations.
Days 61–90: Scale
- Add email and IVR for the same workflows
- Introduce a new use case (e.g., denial classification, refill workflow)
- Strengthen analytics:
- Measure incremental lift (holdouts), cohort effects, and fairness across segments
- Operationalize:
- Runbooks, incident response, and change management processes
Exit criteria: two channels stable, measurable reduction in cost per task, and leadership sign‑off to expand scope.
Measurement: KPIs that matter
Track outcomes, not just activity. A balanced scorecard for AI agents in healthcare automation:
- Access & experience
- First response time; time to resolution; abandonment rate
- CSAT/NPS; language coverage; accessibility compliance
- Containment & quality
- Containment rate by workflow and channel
- Correct action rate (policy adherence); escalation rate and reasons
- Handoff quality (completeness of context and recommendations)
- Safety & governance
- Privacy incidents; denied unsafe actions; parameter validation failures
- Audit completion; adherence to approvals; change control outcomes
- Financial & operational
- Cost per resolution; denials prevented; days in A/R; revenue captured
- Staff time saved; clinician after‑hours reduction; overtime shifts avoided
- Fairness & reliability
- Performance by language, age group, region
- p95 latency by workflow; system uptime; error taxonomy trends
Tie one decision each week to what the scorecard shows then document the impact.
ROI modeling and examples
Build a conservative model with base/best/worst scenarios.
- Inputs:
- Volume per workflow, containment targets, human vs. automated cost, expected reduction in denials or leakage, subscription/integration costs
- Outputs:
- Annual savings, incremental revenue, payback period, and net ROI
Example (access and RCM bundle):
- 200k scheduling changes/year; $4 human cost; $0.80 automated; 40% containment
- Savings: 200k × 0.4 × ($4 − $0.80) = $256k
- Denial prevention: 10k claims scrubbed, 3% fewer denials × $180 avg. recovery = $54k
- Program cost: $180k (licenses, build, governance)
- Net ROI ≈ ($256k + $54k − $180k) ÷ $180k ≈ 0.72 (72%) in Year 1; higher in Year 2 as scope expands
Your numbers will vary; track real data to refine assumptions quarterly.
Operating model: who does what
Successful programs assign clear roles.
- Executive sponsor:
- Aligns goals, budget, and cross‑functional support
- Clinical safety lead:
- Approves clinical policies, escalation, and disclosures
- Compliance/privacy officer:
- Oversees HIPAA/Part 2; DPAs, audits, and vendor risk
- Product owner:
- Prioritizes workflows; owns KPIs; drives the roadmap
- Integration/data engineering:
- EHR/payer connectivity; identity matching; logging; security
- Quality and evaluation:
- Golden sets; regression tests; fairness and outcome monitoring
- Frontline champions:
- Provide feedback; co‑design SOPs; help land change management
Meet weekly; review the scorecard; commit to one improvement based on the data.
Vendor selection checklist (build, buy, or hybrid)
When evaluating platforms for AI agents in healthcare automation:
- Guardrails and policy enforcement:
- Allow/deny lists, approvals, parameter validation, kill switches
- Integrations:
- Proven EHR connectors (FHIR/SMART, vendor APIs), X12 support, telephony, CRM
- Observability:
- Traces, cost metrics, quality dashboards, replay tools for audits
- Privacy and security:
- SOC 2/HITRUST, BAAs, PHI redaction, data residency options, BYOK (bring your own keys)
- Evaluation:
- Offline testing, golden set support, canary releases, A/B frameworks
- Product/partner maturity:
- Roadmap, SLAs, uptime history, RPO/RTO commitments
- Pricing:
- Transparent, usage‑aligned; caps and alerts to prevent surprises
- Customer references:
- Similar environments; evidence of outcomes and safe operations
Run a 30‑day pilot with clearly defined exit criteria: containment, CSAT, safety events, and stakeholder satisfaction.
Case snapshots (anonymized)
- Integrated delivery network (access + IVR)
- Scope: Scheduling changes, directions, prep instructions
- Outcome (90 days): 38% containment, −41% average wait time, +3.9 CSAT points; no policy violations
- Regional health plan (RCM + prior auth)
- Scope: Eligibility verification, claims edits, appeal drafts
- Outcome (120 days): 17% fewer avoidable denials, 23% faster appeal cycle; operational savings exceeded subscription by 2.3×
- Multispecialty clinic (documentation + orders follow‑through)
- Scope: Ambient note drafts, order/result tracking, patient nudges
- Outcome (60 days): 2.1 hours clinician admin time recovered per week, 9% more orders completed within window
Results depend on data quality, policy clarity, and disciplined rollout but the pattern is consistent when those are strong.
Common pitfalls (and how to avoid them)
- Ambiguous scope:
- Fix: Define what “resolved” means per workflow; codify exclusions and escalation triggers
- Stale or conflicting knowledge:
- Fix: Quarterly content review; single source of truth; expiration dates on policies
- Weak identity verification:
- Fix: Enforce secure verification before account changes; log and audit access
- Over‑automation:
- Fix: Start with low‑risk, high‑volume tasks; introduce approvals for sensitive actions; measure CSAT by path
- “Black box” decisions:
- Fix: Log rationales, data sources, and policy matches for each action; ensure explainability at audit time
- Ignoring bias and accessibility:
- Fix: Test performance by language and demographic; provide alternative paths; adhere to accessibility standards
- No incident playbook:
- Fix: Triage → contain (disable action/intent) → eradicate (patch policy/tool) → recover → post‑mortem; rehearse quarterly
A little discipline up front prevents a lot of cleanup later.
Future trends to watch
- Real‑time prior authorization:
- Payer APIs and attachments mature; faster determinations with structured documentation
- TEFCA‑enabled data exchange:
- Broader access to clinical histories via QHIN networks supports richer context retrieval
- Stronger write APIs:
- EHR platforms expand safe write scopes; more end‑to‑end workflows in one loop
- Multilingual parity:
- Native‑quality understanding and responses across languages improve equity
- Verified actions:
- Cryptographic signatures and tamper‑evident logs for high‑risk steps
Adopt trends that serve patient outcomes and your KPIs not just what’s shiny.
FAQs: AI agents in healthcare automation
What are the best first workflows for AI agents in healthcare automation?
Eligibility verification, appointment rescheduling, pre‑visit intake, order/result follow‑through, and basic denial classification. They’re frequent, rules‑based, and low risk.
How do we ensure safety and compliance?
Mask PHI in logs, enforce least privilege, add approvals for sensitive steps, and maintain immutable audit logs. Align with HIPAA/Part 2, FDA (where applicable), ONC transparency, and EU AI Act requirements for medical functions.
Do these agents replace staff?
No. AI agents in healthcare automation remove repetitive work and tee up complex cases with context. Clinicians and staff make final judgments, build relationships, and handle exceptions.
How do we prevent incorrect actions?
Use allow/deny lists, parameter validation, confidence thresholds, and step‑up approvals. Require identity verification for account changes. Monitor action logs and run canaries when deploying changes.
What about diagnosis and treatment decisions?
Keep agents in supportive roles unless you’ve met regulatory requirements for medical device software. Non‑device functions (e.g., admin, documentation) carry lower regulatory burden; clinical judgment remains with licensed professionals.
How do we measure success?
Track containment, time to resolution, CSAT, cost per task, denial reduction, revenue captured, and fairness across languages and demographics. Review weekly; adjust scope and policies accordingly.
How do we handle multilingual support?
Combine high‑quality translation and localized content with human review for critical communications. Measure performance parity across languages and provide accessible alternatives.
Build vs. buy?
Buy for speed, guardrails, and mature integrations. Build when you have unique workflows, strict data residency, or strong internal teams. Many organizations use a hybrid approach: a platform for orchestration and in‑house connectors/policies.
How long to see results?
Meaningful wins often appear in 30–90 days for access and RCM workflows. Documentation and care coordination improvements compound over quarters as adherence and throughput rise.
What governance should we set up?
Create a cross‑functional council (clinical, privacy, product, operations) that meets monthly. Review scorecards, incidents, fairness metrics, and scope changes. Treat policies as code with version control and release notes.
Conclusion: Start small, move fast, protect trust
The promise of AI agents in healthcare automation isn’t replacing clinicians it’s removing obstacles that keep them from practicing at the top of their license. With a focused scope, strong guardrails, and a weekly improvement rhythm, you can reduce delays, errors, and administrative drag while improving patient experience and staff well‑being.
Your next steps:
- Identify two to three low‑risk, high‑volume workflows to automate
- Clean and tag your knowledge base; codify policies and approvals
- Stand up guardrails: redaction, allow/deny lists, approvals, and audit logs
- Pilot on chat or portal messages with a golden test set and canary rollout
- Measure containment, TTR, CSAT, and safety; meet weekly to adjust
- Expand to email and IVR once quality holds; add one new workflow per quarter
Do this for one quarter, and you’ll feel the difference: steadier access, fewer denials, less after‑hours admin, and a calmer team. That’s the true value of AI agents in healthcare automation safer, smarter care operations that respect both people and outcomes.
This was a pleasant surprise — high-quality content and useful tips.